
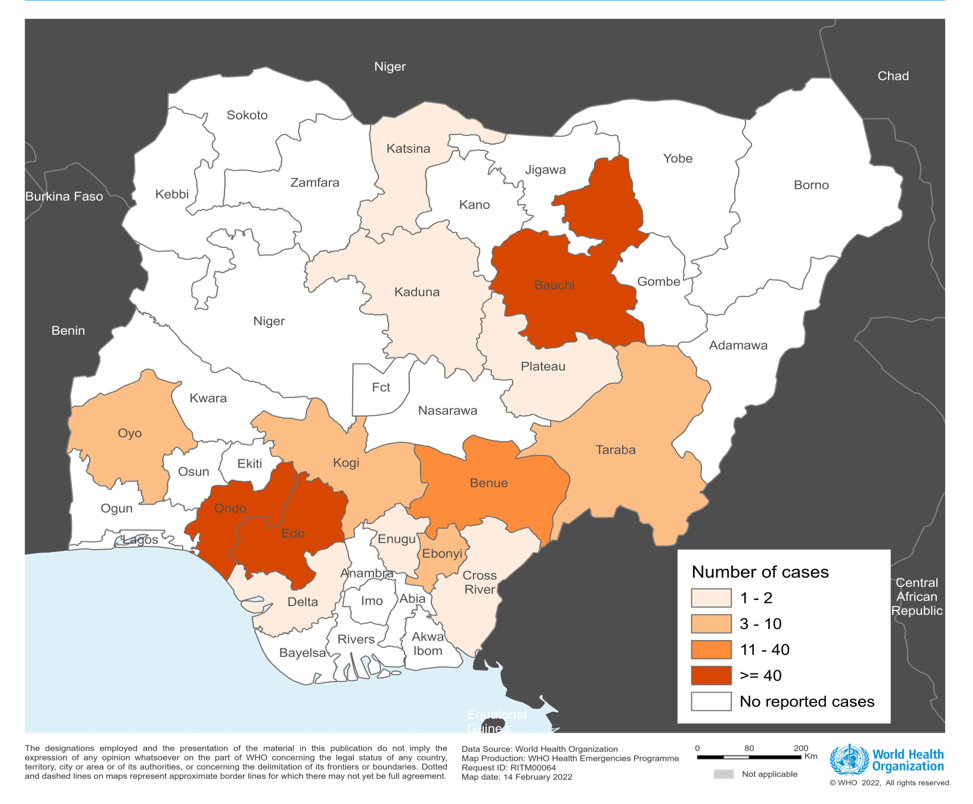
In Nigeria, from 3 to 30 January 2022, 211 laboratory confirmed Lassa fever cases including 40 deaths (case fatality ratio: 19%) have been cumulatively reported in 14 of the 36 Nigerian states and the Federal Capital Territory across the country (Figure 1). Three states account for 82% of confirmed cases: Ondo (63), Edo (57) and Bauchi (53). The other states affected are Benue (11), Ebonyi (5), Oyo (5), Taraba (5), Kogi (4), Enugu (2), Kaduna (2), Cross River (1), Delta (1), Katsina (1) and Plateau (1) (Figure 2).
Of the 211 laboratory confirmed cases, five cases have been reported among health workers in two states, Edo (3) and Benue (2).
In contrast, noticeably less Lassa fever cases with less geographical spread were reported for the same period (epidemiological weeks 1- 4) in 2021 (54 confirmed cases, including 12 deaths, from 8 States).
Lassa fever is endemic in Nigeria and the annual peak of Lassa fever cases is typically observed during the dry season (December–April). Thus, the number of infections is expected to rise further until the end of the dry season.
While endemic in Nigeria, cases are much higher than the previous epidemic seasons. This could be attributed to reduced response capacity in surveillance and laboratory testing. It is necessary to continue to monitor the annual peaks of Lassa fever in order to contextualize incidence and inform the effective management of Lassa fever.
Public health response
- Coordination: The Nigeria Centre for Disease Control (NCDC) has activated the National Emergency Operations Centre alert mode for effective multi-sectoral, multi-disciplinary coordination of the response. Similarly, state public health operation centres were activated in affected states. National rapid response teams (NRRT) have been deployed to the Federal Capital Territory and Bauchi, Benue, Ebonyi, Edo, Nasarawa, Ondo, Oyo and Taraba States.
- Case Management and Infection Prevention and Control (IPC): Case management, and infection prevention and control (IPC) guidelines have been disseminated. Public and health-care worker advisories have been distributed. Case management and IPC training for treatment centre health-care workers have been conducted.
- Surveillance: Enhanced surveillance activities for Lassa fever are ongoing in all states including increased case finding. Reported data is used to generate situational updates by the NCDC and inform further response plans.
- Clinical management: Confirmed cases are being treated at identified treatment centres across the states. Medical response commodities have been distributed to states and treatment centres.
- Laboratory capacity: The seven national Lassa fever laboratories within the NCDC network that can perform molecular tests are working with full capacity to ensure timely processing of samples.
- Community engagement: Risk communications and community engagement activities have been scaled up through television, radio, print, social media and other strategies.
- Vector and environmental control: The Federal Ministry of Environment is implementing a Lassa fever environmental response campaign in affected states.
WHO risk assessment
Lassa fever is a viral haemorrhagic fever that is primarily transmitted to humans via contact with food or household items contaminated with urine or faeces from Mastomys rats. Though to a lesser extent, secondary human-to-human transmission can also occur through direct contact with the blood, secretions, organs or other body fluids of infected persons, especially in health-care settings.
As aforementioned, the peak of Lassa fever cases in humans typically occurs in the dry season (December-April) and follows the reproduction cycle of the Mastomys rats in the wet season (May – November). Given that 90-95% of human infections are due to indirect exposure (through food or household items contaminated by infected rats’ excreta) or direct contact with infected Mastomys rats, the very high density and high circulation of Lassa fever virus in the rat population poses a risk for further human infection during the dry season.
Approximately 80% of Lassa virus infections in humans are either asymptomatic or mild, however, infection in the remaining 20% manifests as a febrile illness of variable severity associated with multiple organ dysfunctions with or without haemorrhage. The overall case fatality ratio among all infected people is approximately 1% but is significantly higher among patients hospitalized with severe illness (around 15%).
Timely diagnosis results in more rapid isolation of patients and provision of treatment, while also reducing the risk of person-to-person transmission in health care settings. Early supportive care with rehydration and symptomatic treatment improves survival of patients.
The current overall risk is considered high at national level. While Lassa fever is endemic in Nigeria and the country has developed an increased capacity for the prevention and control of Lassa fever outbreaks, including strengthened surveillance, diagnostic and treatment capacity, several factors contribute to the current elevated risk level. These include an increase in the number of confirmed cases compared to previous epidemic seasons, gaps in surveillance and varying degrees of subnational response capacity, delays in sample shipment for laboratory testing, a decrease of case management capacity due to conversion of dedicated Lassa fever facilities into COVID-19 health-care facilities and suboptimal IPC procedures. These factors combined warrant the need for further improvement and support of the country’s capacity to detect and respond to Lassa fever outbreaks. In addition, the five confirmed cases among health workers, which included two workers caring for the same patient in the emergency ward, further emphasizes the urgent need to strengthen IPC measures.
The overall regional and global risk is considered low due to minimal cross-border transmission from Nigeria to neighbouring countries. Lassa fever is known to be endemic in West African countries, primarily in Sierra Leone, Guinea, Liberia and Nigeria, but may exist in other countries in the same region.
WHO advice
Mastomys rats are the main reservoir for Lassa virus and so abundant in endemic areas in West Africa that it is not possible to eliminate them from the environment. Prevention of Lassa fever relies on promoting good “community hygiene” to discourage rodents from entering homes. Effective measures include storing grain and other foodstuffs in rodent-proof containers, disposing of waste far from the home, maintaining clean households and considering keeping cats. Precaution should be taken when handling Mastomys rats. All animal products should be thoroughly cooked.
Those caring for affected persons should be careful and avoid contact with blood and body fluids.
In health-care settings, health workers and volunteers should apply standard infection prevention and control (IPC) measures when caring for individuals, regardless of their presumed diagnosis. These include basic hand hygiene, respiratory hygiene, use of personal protective equipment (to block splashes or other contact with infected materials) and safe injection practices.
Health workers caring for those with suspected or confirmed Lassa fever should apply extra infection control measures to prevent contact with the person’s blood, body fluids and contaminated surfaces or materials such as clothing and bedding. When in close contact (within 1 meter) of individuals with Lassa fever, health workers should wear face protection (a face shield or a medical mask and goggles), a clean, non-sterile long-sleeved gown, and gloves (sterile gloves for some procedures).
Personnel working in laboratories are also at risk. Samples taken from suspected Lassa fever cases for diagnostics should be handled by trained staff and processed in suitably equipped laboratories under maximum biological containment conditions.
WHO continues to advise all countries endemic for Lassa fever on the need to enhance early detection and treatment of cases to reduce the case fatality rate.
WHO advises against any restrictions on travel or trade to or from Nigeria and the affected areas based on the currently available information
Source: https://reliefweb.int/report/nigeria/disease-outbreak-news-lassa-fever-nigeria-14-february-2022